The Unclaimed People Buried in St. Francis Hospital Cemetery
There are just under 4,000 patients listed in the five St. Francis Hospital Burial Registers which cover the burials of unclaimed patients who died in the Hospital between the years of 1860 to 1953. The cemetery consists of two adjoining burial grounds. The first burial ground was used from 1860 to 1891 and accounts for the first (by date) 1,671 entries in the burial registers. The second burial ground, roughly the same area as the first, was used from 1892 to 1953 and accounts for 2,221 entries in the burial registers. Each burial ground is a rectangle of approximately 1.25 acres. The top northeast corner of the first is joined by the bottom southwest corner of the second burial ground.
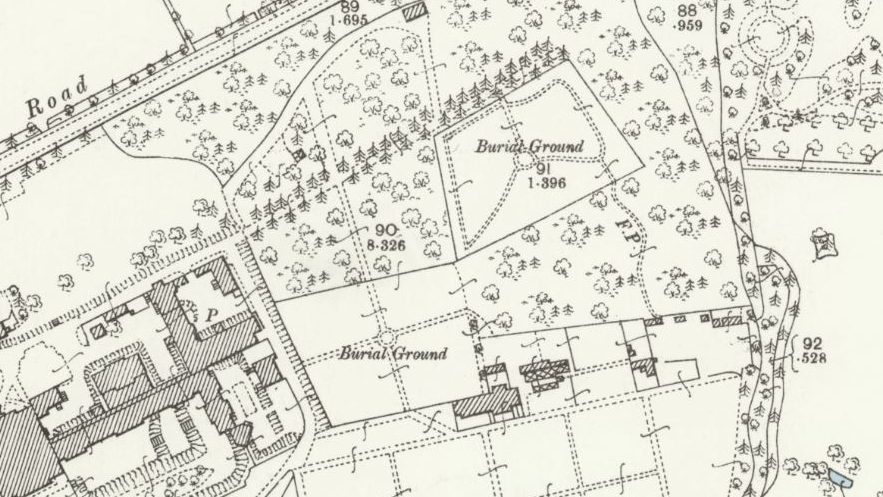
1892-1914 OS map showing the locations of the burial grounds in relation to the main building (left)
Today, the northeastern corner of the 2.5 acre cemetery is about 125 metres roughly south west from the main entrance to the Princess Royal Hospital, Haywards Heath. There is no indication that almost 4,000 mental health patients from the old St. Francis hospital lie buried so close to the main entrance to the hospital.
The first burial in the cemetery was on 3rd September 1860, for Edward Jenner, age 42, Last Place of Abode, Lewes. The last burial in the cemetery was on 27th August 1953, for Louisa Fairhall, age 65, Last Place of Abode, 22 Carlton Place, Brighton.


For the people buried in the cemetery, the average (mean) age at death is 54.52, the median (mid-point) age at death is 56, the mode (most frequent) age at death is 70.
The workhouses in the County of Sussex (and a few other workhouses from other counties) according to the Last Place of Abode entries in the burial registers, tell us that 22.51% of the people buried in the cemetery were admitted to St. Francis Hospital from a workhouse.
About 95% of the people in the cemetery had their Last Place of Abode listed in their burial record as being in somewhere in Sussex. Occasionally through the period in which St. Francis Hospital was functioning of people came into the hospital in groups from other hospitals or even Workhouses that were in other counties. An example of this was in the very early 20th century when 110 patients arrived in St. Francis Hospital from Cardiff in 1904 where the Cardiff City Asylum did not open until 1908 and mental health beds were badly needed because the Cardiff Workhouse and the Glamorgan Asylum were overcrowded in 1904, presumably with people with mental health difficulties. St. Francis Hospital had the space to take these patients as the new East Sussex Asylum at Hellingly near Eastbourne opened in 1903. As this Asylum opened it took East Sussex residents from St. Francis Hospital, which by chance released patient beds which came in very useful when beds were needed by the Cardiff patients, who were duly drafted in. Quite a few of these Cardiff people must have been in poor physical shape as by the end of March 1908 53 of the people, almost 50% in the 1904 draft, were dead and buried in St. Francis Hospital cemetery. But as stated earlier 95% of the people in St. Francis cemetery came from Sussex. We can assume that approximately the same percentage of St. Francis patients were also from Sussex. And these people were mainly dependent on employment in Sussex and the vicissitudes that accompanied life in Sussex.
In the period in which St. Francis Hospital was opened, 1859 until about 1900 there were great changes in the employment profile of people in Sussex as the use of land started to change and as the railway lines grew in use and popularity.
The following section in italics is provided thanks to Google:
Between the mid-19th and early 20th centuries, agriculture and related industries were the primary sources of employment in Sussex, particularly in West Sussex. Many residents worked on farms or in occupations dependent on agriculture, such as brewing, food processing, and milling. Additionally, domestic service was a significant source of employment, with many middle and upper-class families employing servants. The development of seaside resorts also created new jobs in the service industry.
Here’s a more detailed breakdown:
- Agriculture:
Sussex, especially West Sussex, remained largely agricultural during this period, with a focus on farming and related activities.
- Great Estates:
Large estates owned by the aristocracy were major employers, providing work in farming and household management.
- Domestic Service:
The demand for domestic servants was high in the Victorian era, providing employment for many.
- Seaside Resorts:
The growth of seaside resorts like Bognor, Littlehampton, and Worthing created jobs in the service sector, such as hotels, shops, and entertainment.
- Railways:
The expansion of the railway network provided employment opportunities for construction and maintenance of the lines.
We expect that as more stories about people in St. Francis Hospital cemetery are published, we will get an increasing insight into the lives of people in Sussex as things changed around them over the years. We may see how these changes might have affected people’s mental health which in turn will have an effect on the lives of the people around them, mainly members of their own family. We will meet many Agricultural Labourers, Farmers and other people whose lives involved working on the land, Domestic Servants and other workers who earned their living in the homes of middle and upper class people, people who worked in the seaside holiday towns, people who worked on the estates, on the railways and at sea. We will meet these people when they are young and see most of them progress to their middle and late years. Hopefully we will see the benefits of mandatory education, of the growth of national social security, of national pension schemes, and eventually perhaps of the National Health Service. We will see the effect on family life of the losses of people in WW1 and perhaps WW2. We might see the terrible effects on mental health on the men who fought in WW1 and WW2.
The relentless physical AND mental stress of everyday life drove many people in to the County Asylums of the UK in the latter part of the 19th century and the early part of the 20th century. And having been committed to an Asylum they might have been quite difficult for a patient to leave for good. Let’s have a look at two sets of statistics that can show us the differences between UK family life then and now. The first is UK child mortality rate between 1860 (the year after the Sussex Asylum opened) and 2020. In 1860 about 260 out of each 1,000 child births resulted in death before reaching 5 years. In 2020 this rate had improved to just 4 child deaths per 1,000 live births. (With thanks to https://www.statista.com/statistics/1041714/united-kingdom-all-time-child-mortality-rate/ ) Imagine the emotional stress on families when the infant mortality rate was so high and the birth rate so high compared to today.
Another example of life-affecting improvement between then and now, but this time going back a bit less than 50 years – in 1974 there were about 660 fatal injuries in UK workplaces, by the 2020s this had dropped to about 130. (With thanks to https://www.statista.com/statistics/292272/fatal-injuries-at-work-great-britain-by-employment-y-on-y/ ) I can find no comparative figures for the Victorian period in the UK but I’m sure that the fatality rate (let alone the serious injury rate) was far higher than in the 1970s. In the 2020s we have far fewer workers and far better health and safety legislation than we had for the comparative workforce in heavy industry manufacturing, (often called “metal bashing”), and also in ship building, fishing, coal mining, cotton mills and farming in 1860. I am assuming that there were far more workplace fatalities back then there are now and perhaps less recording of these deaths as work place fatalities. Imagine what this unknown, but probably huge by comparison, workplace fatality list did to family income and emotional wellbeing when compensation from employers and government was either non-existent or almost insignificant. And when the bread winner for the family died young the Workhouse beckoned, perhaps quickly followed by the Asylum. Another level of emotional stress that it is hard to imagine today.
And in the time period in which we are doing our researching there was no comprehensive National Health Service, no social security safety net that we would recognise today, no comparable employment protection, no comparable health and safety legislation, no comparable tenancy legislation, no comparable pensions legislation, no comparable child protection legislation, no comparable education legislation etc. etc. and very few charitable institutions that working people could go to get help for family members with mental health problems or learning difficulties. The family had to “soak up” the problems and handle them within the immediate or wider family group. This further added to the huge stresses of everyday life for working people. Stress was often shared and therefore had an increased range. And all this in a period when “Britannia Ruled the Waves”, “The sun never set on the British Empire” etc. What percentage of the population had the vote then and how does this compare to today? Did working people feel trapped and on a relentless treadmill? Can we imagine the cumulative mental health impacts on the family life of working people in the period in which St. Francis Hospital was functioning?
The following sections in italics are provided thanks to Google and its AI use: Please take some time to read these sections and as you absorb them mentally think about the potential stress factors indicated in the previous few paragraphs.
What causes MENTAL HEALTH PROBLEMS?
Mental health problems arise from a complex interplay of factors, including biological, psychological, and social influences. These factors can be broadly categorized as:
- Biological Factors:
Genetics, brain chemistry (neurotransmitters), and physical health conditions can contribute to mental health problems. For example, a family history of depression or anxiety can increase an individual’s risk.
- Psychological Factors:
Personal beliefs, coping mechanisms, past experiences, and even personality traits can influence mental health.
- Social Factors:
Relationships, family dynamics, cultural norms, socioeconomic status, and stressful life events can all impact mental well-being.
Specific Factors Contributing to Mental Health Problems:
- Trauma and Abuse:
Experiences like childhood abuse, neglect, or witnessing violence can have long-lasting effects on mental health.
- Stressful Life Events:
Major life changes, such as losing a job, experiencing financial difficulties, or dealing with relationship issues, can trigger or worsen mental health problems.
- Substance Abuse:
Drug and alcohol misuse can both cause and exacerbate mental health issues.
- Social Isolation and Loneliness:
Lack of social support and feelings of isolation can negatively impact mental health.
- Chronic Medical Conditions:
Physical illnesses, particularly those that are chronic or debilitating, can have a significant impact on mental well-being.
- Genetics:
Some mental health conditions have a strong genetic component, meaning they can be passed down through families.
- Brain Function:
Imbalances in brain chemistry, such as neurotransmitter levels, can contribute to mental health problems.
- Environment:
The physical and social environment, including factors like noise, natural light, and social surroundings, can also affect mental health.
Examples of Mental Health Problems:
- Depression: Characterized by persistent sadness, loss of interest, and fatigue.
- Anxiety: Marked by excessive worry, fear, and nervousness.
- Post-Traumatic Stress Disorder (PTSD): Develops after experiencing a traumatic event.
- Bipolar Disorder: Involves periods of mania (high energy) and depression.
- Schizophrenia: A chronic mental illness characterized by disruptions in thinking, perception, and behaviour.
It’s important to remember that mental health is a complex issue, and the causes of mental health problems are often multifaceted. Seeking help from a mental health professional is crucial for diagnosis and treatment.
LEARNING DIFFICULTIES: Are we born with them or do we acquire them in life?
Learning disabilities can be present at birth or develop later in life. They are often linked to brain development issues that occur before, during, or shortly after birth. However, learning disabilities can also be acquired due to brain injuries or illnesses later in life.
Causes:
- Genetic factors:
Certain inherited conditions can increase the risk of learning disabilities.
- Prenatal factors:
Conditions like infections, maternal substance use, or lack of oxygen during pregnancy can affect brain development.
- Birth complications:
Premature birth, trauma during delivery, or low birth weight can also contribute.
- Early childhood illnesses or injuries:
Conditions like meningitis or brain injuries can affect brain development.
- Acquired brain injuries:
Brain injuries sustained later in life, such as from a fall or accident, can result in learning disabilities.
LEARNING DIFFICULTIES – In Summary
While many learning disabilities are present from birth or develop in early childhood due to factors affecting brain development, they can also be acquired later in life through brain injuries or illnesses.
